The final report from the National Health Service Cass Review has been met in Australia with a concerted propaganda effort claiming that the report has no relevance here.
This is a ludicrous claim.
The water may swirl down the plughole in the opposite direction in the antipodes, but the lack of evidence for so-called ‘gender affirming care’ applies equally in both hemispheres.
Genspect Australia has written to all Australian Health Ministers, and politicians Australia-wide to debunk the misinformation, and explain why we need to urgently implement the Cass Review recommendations in Australia:
May 20th 2024
Dear Australian Health Ministers,
Re: Critical relevance of the NHS Cass Review to Australian clinical practice
The recent Final Report of the Cass Review, England’s NHS-commissioned Independent review of gender identity services for children and young people [1] needs to be immediately adopted in Australia because:
The Cass Review has shown there is no good evidence supporting safety or efficacy of ‘gender affirming care’ for children as it is practiced in Australia.
Clinical practice in Australia lies far outside the recommendations of the Cass Review.
The treatment of children and young people with gender-related distress in Australia is even more radical than it ever was in England.
Australia has no NHMRC-approved guideline for care for gender-related distress.
In the absence of an approved Australian guideline, there is precedent that Australian clinicians fall under UK NHS guidance.
Australian children and young people are being put at grave health risk by current unevidenced clinical practices; the Cass Review Final Report is the most thorough review of global evidence, allowing immediate reform in Australia.
Cass Review finds a lack of evidence supporting gender transition.
The Cass Review was initiated following concerns raised by multiple whistle blowers from the Tavistock Gender Identity Development Service (GIDS) in England. The Final Report by Dr Hilary Cass OBE, former President of the UK Royal College of Paediatrics and Child Health, found the evidence base for ‘gender affirming care’ is “remarkably weak” [1].
The UK National Institute for Health and Care Excellence (NICE) and The University of York performed systematic reviews of the evidence for ‘gender affirming care’ for children and young people. As summarised by the Cass Review, they found that there is no good quality evidence for either the safety or efficacy of puberty blockers and cross-sex hormonal treatments. Notably, there is no evidence that these treatments reduce suicide risk [1], despite frequent claims that the treatment is ‘life-saving’.
In response, the NHS now prioritises psychotherapy to help gender confusion in adolescents, and puberty blockers will be restricted to high quality clinical research trials in England [2]. Cross-sex hormones are to be used with extreme caution in people aged 16 to 18 years with approval from an independent panel required. The Cass Review cautions that social transition is an active intervention and may change the trajectory of gender identity development.
This has left Australia’s health services operating outside of the newly established global best practice for supporting gender confused children and young people, as puberty blockers and cross-sex hormones are prescribed at alarming rates [3] and social transition is automatic in Australian clinics.
Australia does not practice what the Cass Review recommends
The assertion has been made in the media that Australian gender clinics are already doing what Cass recommends because we have ‘multidisciplinary’ teams. This is a smokescreen to distract from the ongoing drug prescriptions and surgeries that completely contradict Cass Review recommendations. Please see the addendum below for an explanation of the deceptive nature of this argument.
‘Gender affirming care’ as practiced in Australian children’s gender clinics involves immediate affirmation of a child’s professed gender with change of name and pronouns, followed by puberty blocking drugs from around age 10, cross sex hormones from as young as 14, advice on breast binding, and possible later mastectomy or genital surgery. Immediate affirmation renders multi-disciplinary teams obsolete, and there is no diagnostic process. The contributions of autism, trauma, depression, anxiety, sexual abuse, and failure to accept a developing same-sex attraction to the adoption of a ‘trans’ identity are not considered. The automatic affirmation of children’s professed identities followed by hormonal treatment lies far outside the holistic approach proposed by the Cass Report.
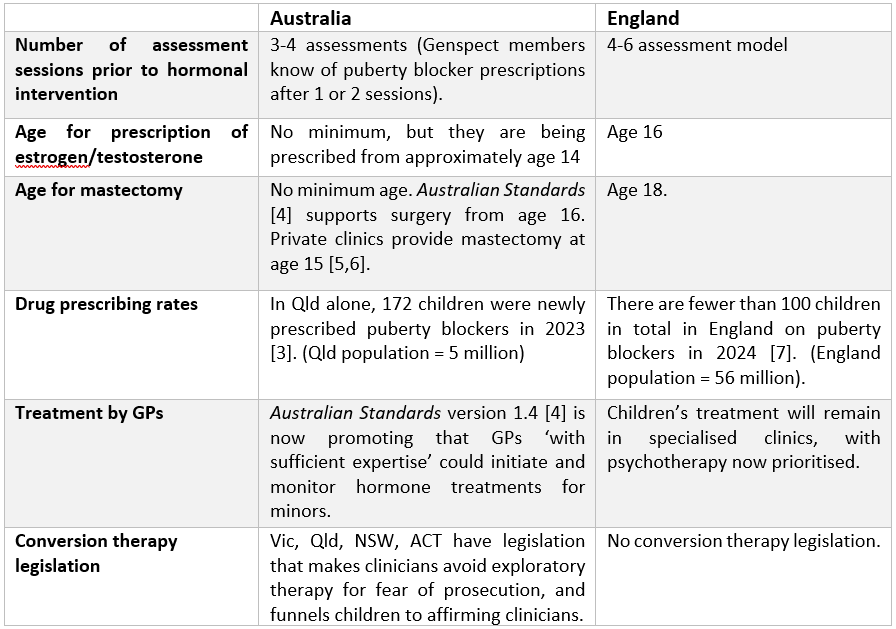
Australia has adopted a more radical approach to ‘gender affirmation’ than England
Genspect Australia is an active group of Australian clinicians, parents and detransitioners with experience in the operation of ‘gender affirming care’ in Australia. Australian paediatric gender clinics are beset by the same problems that the Tavistock GIDS experienced. In fact, Australia has adopted a much more radical form of ‘gender affirming care’ than the Tavistock GIDS:
Australian guidelines are rated as very low quality
Practice in Australia is guided by the ‘Australian Standards of Care and Treatment Guidelines for trans and gender diverse children and adolescents’ [4,8]. The Standard is not of an adequate quality to be considered for inclusion in the Australian Clinical Practice Guideline maintained by the NHMRC. “At the screening stage, it was determined that the guideline did not include a funding statement, an evidence base for the recommendations or information about conflict of interest, and that it would not meet the portal selection criteria, so a full assessment was not carried out,” an NHMRC spokeswoman told The Australian in 2021 [9].
The Cass Review commissioned a systematic review of guideline quality for 23 global guidelines for managing gender dysphoria/incongruence. The Australian Standards of Care received a failing grade of 19% for rigour of development (indicating poor use of an evidence base) and rated poorly overall [10]. The World Professional Association for Transgender Health (WPATH) guidelines are also of low quality [10]. It is completely unacceptable that Australian children are being treated under such poorly respected and unevidenced guidelines. In the absence of adequate local guidelines, we must default to the superior NHS guidance. Please also see the Genspect vision and guidance for responsible care in The Gender Framework [11].
NHS provides the default for Australian clinical guidance
It is easily arguable that our clinicians are already subject to the NHS Cass Review recommendations; there are policy precedents that where Australian clinical guidelines are lacking our clinicians should refer to the NHS for its renowned National Institute for Health and Care Excellence reviewed evidence-base. For example, since the Australian 2013 clinical guidelines for management of borderline personality disorder were rescinded in 2018, the NHMRC has referred clinicians to the NHS guidelines.
Conclusion
The Cass review has determined that practices of puberty blocker and hormonal treatment that are ongoing in Australian children’s gender clinics lack evidence for efficacy and safety. The assertion in the media that our clinics already achieve what Cass aims for is incorrect. We are witnessing a massive failure of medical regulation. There is currently an uncritical governmental acceptance of the opinions of self-appointed experts including AusPATH. There are legitimate dissenting clinical opinions, however, many clinicians are intimidated into silence by aggressive activist groups who seek deregistration of clinicians questioning ‘gender affirming care’.
We call for the immediate implementation of Cass Review Final Report recommendations in Australia.
We have the following specific questions:
Do you agree that Australian children and young people with gender related concerns deserve to be treated according to evidence-based protocols, or in the absence of evidence, under protocols that avoid long term medical harm?
Do you agree that the Australian Standards of Care from the Royal Children’s Hospital Melbourne [4] should not be used, given their (i) low quality, with failure to consider the evidence base [10]; (ii) failure to satisfy NHMRC criteria?
Clinical experts from Genspect Australia would welcome the opportunity to meet with you and discuss the implementation of the Cass Review findings.
Yours faithfully,
The Genspect Australia Committee
References
NHS Cass Review (2024) Independent review of gender identity services for children and young people: Final report.
Amos AJ (2024) Rapidly expanding gender-affirming care based on consensus instead of evidence justifies rigorous governance and transparency. Australasian Psychiatry. doi: 10.1177/10398562241249579.
Telfer MM et al. Australian Standards of Care and Treatment Guidelines for trans and gender diverse children and adolescents Version 1.4. Melbourne: The Royal Children’s Hospital.
Lane, B (2024) ‘Happy day’ An Australian mother shares news that the gender clinic has found a surgeon to perform a double mastectomy on her 15-year old daughter.
Parry J (2024) NHS England to stop prescribing puberty blockers. BBC 13th March 2024.
Telfer MM et al. (2018) Australian standards of care and treatment guidelines for transgender and gender diverse children and adolescents. The Medical Journal of Australia 209: 132-136. See also Telfer MM et al. (2020) Australian Standards of Care and Treatment Guidelines for trans and gender diverse children and adolescents Version 1.3. Melbourne: The Royal Children’s Hospital.
Lane B (2021) Trans lobby ‘buries’ defence of hormone drugs. The Australian.
Taylor J et al. (2024) Clinical guidelines for children and adolescents experiencing gender dysphoria or incongruence: a systematic review of guideline quality (part 1). Archives of Disease in Childhood. doi: 10.1136/archdischild-2023-326499.
Genspect (2023) Gender Framework: A Vision for Change. The Killarney Group. Released for consultation, The Bigger Picture Conference, Denver, Colorado.
Addendum:
Arguments that the Cass Review is not relevant in Australia as our clinics are ‘multidisciplinary’ are misleading.
Genspect is aware of recent media reports claiming that the findings of the Cass Review Final Report are not relevant to Australia because Australian paediatric gender clinics are ‘multidisciplinary’ and ‘holistic’.
We note that the service specification for the UK’s gender clinic similarly described the clinic as ‘multidisciplinary’, ‘holistic and ‘tailored to the needs of the individual and their family/carers’. Consequently it cannot be argued that this is a point of difference between practice in Australia and England that negates the relevance of the Cass Review to Australia.
The claim that Australian paediatric gender clinics are multidisciplinary is misleading. Australian gender clinic clinicians are required to provide interventions according to the affirmation model. This cancels out any benefit from employing clinicians from different professional backgrounds. For example, a speech pathologist employed in a gender clinic provides masculinising or feminising vocal training but does not provide general communication assessments and speech pathology interventions. Similarly, the endocrinologist in the gender clinic team only prescribes puberty blocker and cross-sex hormones and does not provide treatment for any hormonal conditions. Therefore, the restricted model of care in Australian paediatric gender clinics is depriving their patients of comprehensive multidisciplinary assessment and treatment for the various pre-existing and co-occurring conditions contributing to their condition. This approach does not align with the recommendation of the Cass Review Final Report that care for gender dysphoria shouldnot be based on the ‘gender-affirming’ model but instead treat children with gender distress similarly to children with other developmental struggles.
Australian paediatric gender clinics are not ‘holistic’. They provide a very narrow scope of intervention: gender affirming interventions for children with gender dysphoria. They do not deliver any other care or treat any other condition. Specifically, they do not provide broader types of management, such as ADHD support, mental health care, family therapy, or management of underlying endocrine problems. Australian paediatric gender clinics outsource any required psychological therapy to private psychologists in the community which prevents any integration of psychological and medical care.
Focussing on the ‘multidisciplinary’ aspect is a tactic to distract from the issue of hormonal interventions. The central findings of the Cass Report that there is no good evidence to support puberty blocker and hormonal treatment is unaffected by whether or not clinics are multidisciplinary. Australian clinics continue to treat children with puberty blockers and hormones without an evidence base, and are in no way consistent with the recommendations of the Cass Report.
To follow and support the work of Genspect in Australia, consider becoming a free or paid subscriber.
You can join Genspect Australia through the website portal.