


Human Rights Conventions in relation to gender medicine in New Zealand.
Human Rights Conventions in relation to gender medicine in New Zealand.
Genspect is an international alliance of parents and professional groups who advocate for a non-medicalised approach to gender diversity. Our members also include concerned trans people and detransitioners, whose contribution informs our activities. We number in our thousands, including increasing numbers in New Zealand. Genspect New Zealand contributors include health policy experts and clinicians including psychotherapists, general practitioners, and hospital specialists, many of whom have been involved in treating individuals with gender confusion. We also have parents whose children have attended child or adult gender clinics and are very familiar with the practice of gender medicine in New Zealand. We represent the interests of gender confused youth as well as concerned clinicians and parents. Disturbingly, the majority of clinicians fear negative assessments and career implications if they speak out regarding the medicalisation of ‘affirmative care’(Dashfield, 2024; Paul, 2023) and parents fear losing contact with their children if they express their concerns publicly. We speak for them.
The purpose of this paper is to examine the existing human rights framework to understand how it would protect children, young people, and vulnerable adults in the light of the findings from the Cass Report (Cass, 2024a).
New Zealand is a signatory to a number of human rights treaties which provide an agreed set of human rights standards. These provide important guidance to governments and organisations on their obligations to act in certain ways, or to refrain from certain acts in order to promote and protect human rights and the fundamental freedoms of individuals or groups.
A human rights framework that promotes the freedom and autonomy of individuals incorporates provisions to ensure that such freedoms do not impact on the rights of others (see Article 29(2) of the Universal Declaration of Human Rights). New Zealand is signatory to conventions that include consideration of the rights of children and the need to protect them from harm. This includes the child’s inability to consent to medical interventions with potentially life-long impacts. As stated in the UN Declaration of the Rights of the Child, "the child, by reason of his physical and mental immaturity, needs special safeguards and care, including appropriate legal protection, before as well as after birth"(United Nations, 1998). Therefore, adult rights to freedom and autonomy in respect of medical treatments for gender issues should not be automatically conferred to children and adolescents.
Genspect New Zealand considers that the provision of so-called ‘gender-affirming care’ in New Zealand represents one of the greatest current threats to the human rights of children and young people. Specifically these include gender non-conforming young people who are highly likely to mature as same sex-attracted adults, and children who have faced significant trauma or who have autism syndrome conditions (Counties Manukau DHB, 2011; Singh et al., 2021; Vrangalova, 2017). The ‘gender affirming” treatments given to children and young people lack evidence for safety and efficacy (Cass, 2024a), and violate the following provisions of human rights conventions to which New Zealand is a signatory:
United Nations Convention on the Rights of the Child (CRC) (1989)
Article 3 (3): Parties shall ensure that the institutions, services and facilities responsible for the care or protection of children shall conform with the standards established by competent authorities, particularly in the areas of safety, health, in the number and suitability of their staff, as well as competent supervision (UNICEF, 1989).
Commissioned by the UK’s National Health Service, the Cass Review Final Report, published on 10 April 2024 (Cass, 2024a) conducted eight independent systematic reviews of the global research literature to underpin its recommendations (Kingdon, 2024). It reveals there is no clear evidentiary basis for medical ‘gender affirmation’ interventions in children and confirms that the evidence for social conversion, puberty suppression and cross-sex hormone treatment is of such poor quality that no foundation exists for clinical decisions and informed consent.
Concern about the human rights implications of the findings of the Cass Review was raised by Reem Alsalem, who is the United Nations Rapporteur on violence against women and girls, and its causes and consequences: “While the Cass Review may not have framed its conclusions and findings explicitly in human rights language, it has – in my view – very clearly shown the devastating consequences that policies on gender treatments have had on human rights of children, including girls. These policies have breached fundamental principles, such as the need to uphold the best interest of the child in all decisions that affect their lives, and the right of children to the highest attainable standards of health”(Alsalem, 2024).
In New Zealand paediatric gender medicine is highly devolved to hospital-based gender clinics, youth clinics and increasingly to primary care practices. All are yet to conform to the clinical standards established by the competent authority of the Cass Review Final Report. Ancillary services such as psychology, counselling and psychotherapy, like the clinicians themselves, are committed to professional standards that continue to provide interventions based on two documents that were given failing grades on ‘Rigour of Development’, ‘Editorial Independence’ and ‘Applicability’ by the Cass Review – the WPATH Standards of Care 8 (Coleman et al., 2022), and the New Zealand Guidelines for gender affirming healthcare for gender diverse and transgender children, young people and adults in Aotearoa, New Zealand. (Oliphant et al., 2018; Taylor et al., 2024a). As these documents are not competent authorities on health care, consequently, the model of care currently provided in New Zealand is in breach of Article 3(3) in the CRC (UNICEF, 1989).
The CRC clearly places responsibility and care for children with their parents and not the state. A case study of Canada’s response to the CRC argues that the government has ignored the provisions that call for parental nurturance, parental culture and parental responsibility in its local enactments and policy (Genspect, 2023). These considerations are highly relevant in New Zealand where legislation and policy has diminished this relationship in similar ways to Canada.
International Covenant on Civil and Political Rights
Article 7: No one shall be subjected to torture or to cruel, inhuman or degrading treatment or punishment. In particular, no one shall be subjected without his free consent to medical or scientific experimentation(OHCHR, 1966).
Dr Hilary Cass, the paediatrician commissioned to conduct the review discussed above, has said that while doctors tend to be cautious in implementing new findings in emerging areas of medicine, “quite the reverse happened in the field of gender care for children” and that gender medicine is “built on shaky foundations” (Cass, 2024b).
On 12 March 2024, the NHS England announced that from 1 April 2024 they would no longer routinely prescribe puberty blockers. This decision has been confirmed by the incoming UK Labour Government (Law Society of Ireland, 2024) and has comprehensively defeated a legal challenge (BBC News, 2024). The NHS stated: “We have concluded that there is not enough evidence to support the safety or clinical effectiveness of puberty suppressing hormones to make the treatment routinely available at this time. “Puberty blockers will only be available in future, as part of a research trial(Campbell, 2024).
The Cass Review Final Report similarly found that evidence of benefit from puberty blockers was lacking: “no changes in gender confusion or body satisfaction were demonstrated. There was insufficient/inconsistent evidence about the effects of puberty suppression on psychological or psychosocial wellbeing, cognitive development, cardio-metabolic risk, or fertility” (Cass, 2024a).
Regarding masculinising/feminising hormones, the Cass Review found: “There is a lack of high-quality research assessing the outcomes of hormone interventions in adolescents with gender confusion/incongruence, and few studies that undertake long-term follow-up. No conclusions can be drawn about the effect on gender confusion, body satisfaction, psychosocial health, cognitive development, or fertility. Uncertainty remains about the outcomes for height/growth, cardiometabolic and bone health. There is suggestive evidence from mainly pre-post studies that hormone treatment may improve psychological health, although robust research with long-term follow-up is needed.”(Taylor, 2024b).
Therefore, whilst puberty blockers continue to be provided outside of an ethics-approved clinical research trial in New Zealand, and cross-sex hormones are prescribed to minors, children are being subject to medical experimentation at an age when they are unable to provide free and informed consent because they are unable to comprehend the implications of lifelong infertility, impairment in sexual functioning, and serious physical health problems.
The portrayal by gender identity advocates of treatment for gender confusion as social justice and therefore a rights issues is also problematic. New Zealand’s guidelines ascribe the high levels of co-morbid mental health conditions suffered by people seeking gender transition treatment to external factors, citing the theorised existence of minority stress as the cause (Oliphant et al., 2018). However, published data shows the high rates of co-occurring mental health and developmental conditions amongst those presenting to gender clinics (Kozlowska et al., 2021) making it implausible that this is an adequate explanation (SEGM, 2021). The Cass interim report (Cass, 2022) recognised that there are many factors that lead to someone claiming a gender identity that differs from their sex. The final report wrote that “early audits and research suggest that adverse childhood events are a predisposing factor while recognising there are complex interrelationships between identity and mental health". Australian research into child and adolescent gender clinic clients found a high correlation between adverse childhood events and gender questioning (Kozlowska et al., 2021). However, the Cass report also showed that clinicians cannot determine who will benefit from treatment and noted that without treatment the majority of children grow out of their gender identification by the end of puberty.
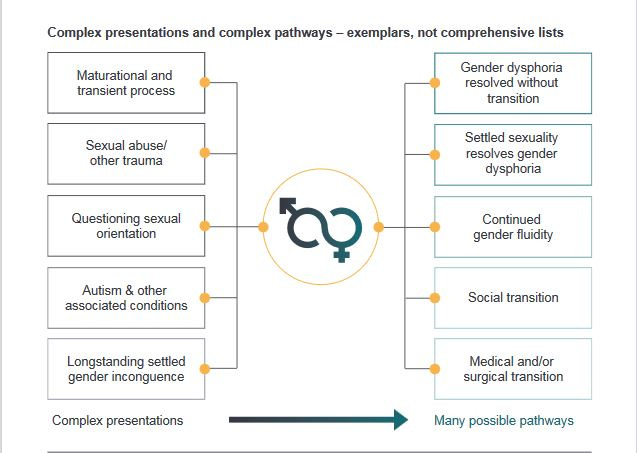
Figure 1 Cass Interim Review diagram shows complex presentations and pathways related to gender identity
It is highly likely that a significant proportion of the children being subject to such medical experimentation in New Zealand would have trauma as a causative factor. Genspect’s own assessment is that treating gender confusion as a social justice and not a medical issue can result in “real mental health problems being overlooked in favour of promoting transition as a cure-all (in effect, diagnostic overshadowing)” and that “the focus must shift from promoting group-rights based on identity to one that is centred on the long-term health and well-being of individuals as a whole person” (Genspect, 2023).
There is no greater evidence for efficacy and safety of treatments for adolescents and vulnerable adults than for children (Sharma et al., 2019; Taylor et al., 2024b). In the absence of reliable data on safety, true informed consent cannot be given. Patients are not being informed that they are being given an experimental and unproven treatment, violating Article 7 listed above. Furthermore, New Zealand’s guidelines do not preclude the provision of hormonal treatment and gender surgeries for severely mentally ill patients, and even those unable to verbalise their gender identity(Oliphant et al., 2018). They are thus unable to properly consent, violating the rights of the disabled.
Universal Declaration of Human Rights
Article 16: Men and women of full age, without any limitation due to race, nationality, or religion, have the right to marry and to found a family (United Nations, 1948).
The medical and surgical interventions (puberty blockers, cross-sex hormones, and gender surgeries) delivered to gender confused children and adolescents in New Zealand pose a significant threat to their right to found a family. Puberty blockers are prescribed to gender questioning children from the start of puberty (age 10 to 12) when children, due to mental immaturity, are not able to comprehend the full implications of life-long infertility. Decision-making in children and adolescents tends to be based on short-term factors with longer-term consequences being relatively disregarded. Studies indicate that ~95% of children prescribed puberty blockers go on to take cross-sex hormones(Brik et al., 2020; Carmichael et al., 2020; Wiepjes et al., 2018). Children following this pathway will be permanently infertile. A research article on clients of the Mayo clinic, which is awaiting peer review, has shown destructive effects on the testes (Murugesh et al., 2024). In New Zealand, cross-sex hormones are prescribed to children as young as age 14, and possibly younger (Hill, 2024). Both testosterone in females and oestrogen in males impacts fertility (Cheng et al, 2019) with oestrogen being of particular concern(Carroll et al., 2023).
Therefore, the hormonal and surgical interventions provided by gender services in New Zealand are a threat to the human right of people to found a family.
Convention on the Elimination of All Forms of Discrimination Against Women (1979) CEDAW
Article 10: Parties shall take all appropriate measures to eliminate discrimination against women in order to ensure to them equal rights with men in the field of education and in particular to ensure, on a basis of equality of men and women: (c) The elimination of any stereotyped concept of the roles of men and women at all levels and in all forms of education by encouraging coeducation and other types of education which will help to achieve this aim and, in particular, by the revision of textbooks and school programmes and the adaptation of teaching methods; (United Nations, 1989)
The educational resources used by advocates of gender affirming interventions for children and adolescents, such as the ‘gender unicorn’ and the ‘genderbread person’ rely on regressive sex stereotypes about what it means to be male or female. Curriculum materials introduced under the Relationship and Sexuality Education Guidelines, (Ministry of Education, 2020) feed the idea that some children are ‘born in the wrong body’. The Guidelines advise teaching every child from entry classes onwards that they have preferred pronouns and a gender identity that may differ from their sex. Supporting material from private providers tells students that not only girls have periods and breasts (Family Planning NZ, 2021). Academic surveys ask every child whether they are transgender, or gender unsure (Fenaughty, et al., 2023). These are all forms of discrimination against girls and women who are asked to view being a girl or a woman as ‘an inner feeling’, rather than a biological reality, and to accept that a female ‘gender expression’ is an appallingly restricted range of interests, activities and appearance preferences. This violates article 10 above, and similar concerns apply to boys being presented with rigid stereotypes of manhood.
Such reliance on regressive sex stereotypes risks placing sex-non-conforming children at the beginning of a pathway towards gender interventions that can have serious, long-term consequences as outlined above. The DSM-V criteria for the diagnosis of “gender dysphoria” in Children relies on such regressive sex stereotypes by considering, as evidence for a diagnosis, the child’s clothing preferences and preferences for “toys, games, or activities stereotypically used or engaged in by the other gender” (Nokoff, 2022)
Regarding the diagnosis of gender confusion, the Cass Review Final Report (Cass, 2024a) stated: “Although a diagnosis of gender dysphoria has been seen as necessary for initiating medical treatment, it is not reliably predictive of whether that young person will have longstanding gender incongruence in the future, or whether medical intervention will be the best option for them”. This indicates that there is no scientific foundation for the use of regressive sex stereotypes as the basis for providing poorly-evidenced medical interventions aimed at changing the body of the child. Without such gender stereotypes, children would be able to continue to dress, play and choose playmates without facing the future risks associated with puberty blockers and cross-sex hormones: infertility, lack of sexual function, long-term physical health problems and the risk of regret.
Therefore, the educational resources used by paediatric gender clinics and trans-advocacy organisations that reinforce regressive sex stereotypes as part of an education program about ‘gender identity’ places New Zealand in breach of its commitment to eliminate stereotyped concepts of the roles of men and women at all levels and in all forms of education.
Conclusion
Genspect has identified a number of current and emerging threats to human rights stemming from the ‘gender-affirming’ treatment model provided in New Zealand paediatric and adult gender clinics. Genspect urges immediate action to halt these gender clinic services which are providing experimental medical interventions to children and adolescents, a significant proportion of whom suffer from mental health conditions. Gender interventions are underpinned by regressive sex stereotypes and affect the child’s future ability to found a family.
We urge the government to ensure that gender services for children operate in accordance with New Zealand’s human rights obligations to ensure that health services conform to the standards outlined by a competent authority. The definition of competent authority must include adherence to the best available evidence. Unfortunately, this currently precludes a number of medical bodies in New Zealand that are dominated by activist interests rather than evidence-based medicine(Tegg, 2024). This requires the Government to insist on the implementation of the recommendations within the Cass Review Final Report in New Zealand paediatric gender services.
References
Alsalem, R. (2024). UK: Implementation of ‘Cass report’ key to protecting girls from serious harm, says UN expert. OHCHR. https://www.ohchr.org/en/statements/2024/04/uk-implementation-cass-report-key-protecting-girls-serious-harm-says-un-expert
BBC News. (2024). Puberty blockers ban is lawful, says High Court. BBC News. July 3. https://www.bbc.com/news/articles/c4ng3gz99nwo
Brik, T., Vrouenraets, L. J. J. J., de Vries, M. C., & Hannema, S. E. (2020). Trajectories of Adolescents Treated with Gonadotropin-Releasing Hormone Analogues for Gender Dysphoria. Archives of Sexual Behavior, 49(7), 2611–2618. https://doi.org/10.1007/s10508-020-01660-8
Campbell, D. (2024). Children to stop getting puberty blockers at gender identity clinics, says NHS England. The Guardian. March 12. https://www.theguardian.com/society/2024/mar/12/children-to-stop-getting-puberty-blockers-at-gender-identity-clinics-says-nhs-england
Carmichael, P., Butler, G., Masic, U., Cole, T. J., Stavola, B. L. D., Davidson, S., Skageberg, E. M., Khadr, S., & Viner, R. (2020). Short-term outcomes of pubertal suppression in a selected cohort of 12 to 15 year old young people with persistent gender dysphoria in the UK. Plos One https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7853497
Carroll, R., Sepulveda, B., McLeod, L., Stephenson, C., & Carroll, R. W. (2023). Characteristics and gender affirming healthcare needs of transgender and non-binary students starting hormone therapy in a student health service in Aotearoa New Zealand. Journal of Primary Health Care, 15(2),106–111. https://doi.org/10.1071/HC23040
Cass, H. (2022). Interim report – Cass Review. The Cass Review. https://cass.independent-review.uk/publications/interim-report/
Cass, H. (2024a). Cass Review Final Report. Cass Review. https://cass.independent-review.uk/home/publications/final-report/
Cass, H. (2024b). Gender medicine for children and young people is built on shaky foundations. Here is how we strengthen services. BMJ, 385, q814. https://doi.org/10.1136/bmj.q814
Cheng, P. J., Pastuszak, A. W., Myers, J. B., Goodwin, I. A., & Hotaling, J. M. (2019). Fertility concerns of the transgender patient. Translational Andrology and Urology, 8(3), 209–218. https://doi.org/10.21037/tau.2019.05.09
Coleman, E., Radix, A. E., Bouman, W. P., Brown, G. R., de Vries, A. L. C., Deutsch, M. B., Ettner, R., Fraser, L., Goodman, M., Green, J., Hancock, A. B., Johnson, T. W., Karasic, D. H., Knudson, G. A., Leibowitz, S. F., Meyer-Bahlburg, H. F. L., Monstrey, S. J., Motmans, J., Nahata, L., … Arcelus, J. (2022). Standards of Care for the Health of Transgender and Gender Diverse People, Version 8. International Journal of Transgender Health, 23(sup1), S1–S259. https://doi.org/10.1080/26895269.2022.2100644
Counties Manukau DHB. (2011). Gender Reassignment Health Services for Trans People within New Zealand. https://mohlibrary.softlinkhosting.co.nz/liberty/opac/search.do?mode=BASIC&openDetail=true&action=search&queryTerm=uuid%3D%225e0748bd0a5a01e252669517000416d7%22&editionUuid=5e0748bd0a5a01e252669517000416d7&operator=OR&_open=1
Dashfield, P. (2024). Deafening silence surrounds gender-affirming care. New Zealand Doctor. https://www.nzdoctor.co.nz/article/opinion/deafening-silence-surrounds-gender-affirming-care
Family Planning NZ. (2021). Navigating the Journey: Year 5 and 6 2021
Fenaughty, J., Bavin, L., Choo, W. L., Ker, A., Lucassen, M., Ball, J., & Drayton, B. (2023). Youth19 Rangatahi Smart Survey Initial Finding. Auckland University. https://static1.squarespace.com/static/5bdbb75ccef37259122e59aa/t/653ef9712a382244538fd8f1/1698625910424/Youth19+Gender+Identity+and+young+peoples+wellbeing.pdf
Genspect. (2023). The Gender Framework Draft One. Genspect. https://genspect.org/wp-content/uploads/2023/11/The-Gender-Framework-Draft-One.pdf
Hill, R. (2024). Criticism of puberty blockers misguided, trans girl’s mother says Radio New Zealand, April 21. https://www.rnz.co.nz/news/national/514817/criticism-of-puberty-blockers-misguided-trans-girl-s-mother-says
Kingdon, C. C. (2024). Holistic approach to gender questioning children and young people. Archives of Disease in Childhood. https://doi.org/10.1136/archdischild-2024-327100
Kozlowska, K., McClure, G., Chudleigh, C., Maguire, A. M., Gessler, D., Scher, S., & Ambler, G. R. (2021). Australian children and adolescents with gender dysphoria: Clinical presentations and challenges experienced by a multidisciplinary team and gender service. Human Systems, 1(1). https://doi.org/10.1177/26344041211010777
Law Society of Ireland. (2024). Labour minister backs Tory puberty-blockers ban. Law Society Gazette of Ireland. July 15. https://www.lawsociety.ie/gazette/top-stories/2024/july/labour-minister-backs-tory-puberty-blockers-ban
Ministry of Education. (2020). Relationships and Sexuality Education: Policy Guidelines (11 November). Ministry of Education. https://health.tki.org.nz/Teaching-in-HPE/Policy-Guidelines/Relationships-and-Sexuality-Education
Murugesh, V., Ritting, M., Salem, S., Aalam, S. M. M., Garcia, J., Chattha, A. J., Zhao, Y., Knapp, D. J., Kalthur, G., Granberg, C. F., & Kannan, N. (2024). Puberty Blocker and Aging Impact on Testicular Cell States and Function. bioRxiv: The Preprint Server for Biology, 2024.03.23.586441. https://doi.org/10.1101/2024.03.23.586441
Nokoff, N. J. (2022, January 19). Table 2. [DSM-5 Criteria for Gender Dysphoria]. [Text]. MDText.com, Inc. https://www.ncbi.nlm.nih.gov/books/NBK577212/table/pediat_transgender.T.dsm5_criteria_for_g/
Oliphant, J., Veale, J. F., MacDonald, J., Carroll, R., Harte, M., Stephenson, C., & Bullock, J. J. (2018b). Guidelines for gender affirming healthcare for gender diverse and transgender children, young people and adults in Aotearoa. Transgender Health Research Lab, University of Waikato. https://researchcommons.waikato.ac.nz/bitstream/handle/10289/12160/Guidelines%20for%20Gender%20Affirming%20Health%20low%20res.pdf
OHCHR. (1966). International Covenant on Civil and Political Rights. United Nations. https://www.ohchr.org/en/professionalinterest/pages/ccpr.aspx
Paul, C. (2023). A Terrible Trap. North & South Magazine. Dec 23. https://northandsouth.co.nz/2023/12/24/puberty-blockers-new-zealand/
SEGM. (2021). New Study Raises Questions About the Gender Minority Stress Model. Society for Evidence Based Gender Medicine. https://www.segm.org/Study_Questions_Gender_Minority_Stress_Model
Sharma, R.., Wilson, L., & Baker, K. (2021). Hormone Therapy, Mental Health, and Quality of Life Among Transgender People: A Systematic Review https://academic.oup.com/jes/article/5/4/bvab011/6126016
Singh, D., Bradley, S. J., & Zucker, K. J. (2021). A Follow-Up Study of Boys With Gender Identity Disorder. Frontiers in Psychiatry, 12. https://doi.org/10.3389/fpsyt.2021.632784
Taylor, J., Hall, R., Heathcote, C., Hewitt, C. E., Langton, T., & Fraser, L. (2024a). Clinical guidelines for children and adolescents experiencing gender dysphoria or incongruence: A systematic review of guideline quality (part 1). Archives of Disease in Childhood, archdischild-2023-326499. https://doi.org/10.1136/archdischild-2023-326499
Taylor, J., Mitchell, A., Hall, R., Langton, T., Fraser, L., & Hewitt, C. E. (2024b). Masculinising and feminising hormone interventions for adolescents experiencing gender dysphoria or incongruence: A systematic review. Archives of Disease in Childhood. https://adc.bmj.com/content/archdischild/early/2024/04/09/archdischild-2023-326670.full.pdf
Tegg, S. (2024). Open letter to the New Zealand Health Minister. July 10. https://genspect.org/open-letter-to-the-new-zealand-health-minister/
UNICEF. (1989). Convention on the Rights of the Child Text. UNICEF. https://www.unicef.org/child-rights-convention/convention-text
United Nations. (1948). Universal Declaration of Human Rights. United Nations. https://www.un.org/en/about-us/universal-declaration-of-human-rights
United Nations. (1979). Convention on the Elimination of All Forms of Discrimination against Women. OHCHR. https://www.ohchr.org/en/instruments-mechanisms/instruments/convention-elimination-all-forms-discrimination-against-women
UNICEF. (1989). Convention on the Rights of the Child Text. UNICEF. https://www.unicef.org/child-rights-convention/convention-text
Vrangalova, Z. (2017. There’s Growing Evidence For A Link Between Gender Dysphoria And Autism Spectrum Disorders. Forbes. Nov 15. https://www.forbes.com/sites/zhanavrangalova/2017/11/15/growing-evidence-for-a-link-between-gender-dysphoria-and-autism-spectrum-disorders/
Wiepjes, C. M., Nota, N. M., Blok, C. J. M. de, Klaver, M., Vries, A. L. C. de, Wensing-Kruger, S. A., Jongh, R. T. de, Bouman, M.-B., Steensma, T. D., Cohen-Kettenis, P., Gooren, L. J. G., Kreukels, B. P. C., & Heijer, M. den. (2018). The Amsterdam Cohort of Gender Dysphoria Study (1972–2015): Trends in Prevalence, Treatment, and Regrets. The Journal of Sexual Medicine, 15(4), 582–590. https://doi.org/10.1016/j.jsxm.2018.01.016
Article 16 of the Universal Declaration of Human Rights does not mention people limited by disability.
Transgenderism by its nature disables people, removing fertility. Simply, this is eugenics legally protected by the United Nations.