

Hearing on Puberty Blockers "Like Travelling Back in Time"
Genspect UK Fact Checks the Women and Equalities Committee Hearing on Puberty Blockers

On 22nd January, the UK government’s Women and Equalities Committee (WEC) held an oral evidence session on the safety and effectiveness of puberty blockers. You can read a transcript of the session here.
WEC is not a medical committee. It usually hears evidence on issues like discrimination in the workplace and tackling misogyny, so the evidence base for puberty blockers was a strange choice of topic, particularly given the clear position on blockers laid out by the UK government. Following the Cass Review, which found no evidence to support the use of puberty blockers in treating gender related distress, and a report from the Commission on Human Medicines (CHM) that declared an “unsafe prescribing environment”, Health Secretary Wes Streeting introduced an indefinite ban on their prescription to gender distressed young people in December 2024. Surely the evidence on this issue is settled?
Hilary Who?
But it wasn’t just the topic chosen by WEC that was confusing. The ‘experts’ chosen to give evidence to the committee were puzzling too. The committee has total discretion about who it asks to give evidence, and it might have invited Dr Hilary Cass herself, or a representative from the University of York team who conducted the systematic reviews of puberty blockers that informed the Cass Review. These are people who could truly speak to the complexities and uncertainties of using puberty blockers to address gender related distress.
Instead, the WEC chose to hear evidence from Professor Gary Butler, an endocrinologist instrumental in the scandal that unfolded at the Tavistock Gender Identity Clinic (GIC) and Professor Simona Giordano, a bioethicist and enthusiastic supporter of the disgraced World Professional Association for Transgender Health (WPATH). Professor Ashley Grossman, an adult endocrinologist with no experience of treating gender distressed young people, was apparently included to balance out the unorthodox and partisan views of his fellow speakers.
And their views truly are unorthodox. One might almost say ‘reality defying’. In a speech to the European Professional Association for Transgender Health in 2023, Professor Butler rejected the findings of the Cass Review and denied that there had been any problem with the care delivered by GIDS. He is virtually alone in holding these opinions. GIDS was rated ‘inadequate’ by the Care Quality Commission (CQC) in 2020 and was closed down entirely in 2022 when the Cass Review Interim Report found that the service was unsafe. He also falsely accused Dr Cass of ‘nepotism’, claiming that she had showed favouritism when choosing which hospitals would host the new regional gender identity clinics. In fact, Dr Cass had nothing to do with this decision. Why did the WEC select Professor Butler to give ‘expert’ testimony when he is in denial about well documented safety concerns about the treatment of gender distressed young people?
Similarly, Professor Simona Giordano is a bioethicist with no medical qualifications and the author of papers such as Exploratory psychotherapy: when is psychotherapy a form of conversion?, Lives in a chiaroscuro. Should we suspend the puberty of children with Gender Identity Disorder? and Regret, informed decision making, and respect for autonomy of trans young people. Professor Giordano appears to be a supporter of the informed consent model of treatment, in which preventing young people from undergoing irreversible cosmetic and hormonal treatments is viewed as a violation of their ‘autonomy’, and an effort to ‘convert’ them away from a transgender identity. She is also a supporter of WPATH, a discredited organisation that believes children should be able to medically transition at any age and which advises clinicians to provide castration surgeries to people who identify as ‘eunuchs’. Given all that we now know about the harms of medicalising gender related distress, why did the WEC choose to hear from someone whose views are so completely at odds with the evidence?
I attended the WEC session as Director of Genspect UK, alongside colleagues from Transgender Trend, CAN-SG and the LGB Alliance. Detransitioner Keira Bell was there too. Professor Butler is the endocrinologist who prescribed her the puberty blockers and hormones that she now regrets taking, and Keira brought an entire judicial review against the Tavistock in 2020 on the basis of its unsafe practices and lax safeguarding. I don’t know how she kept her cool during the WEC session. Professors Butler and Giordano claimed repeatedly that there is no evidence that anyone has ever regretted taking puberty blockers, all while Keira sat right behind them, living proof that that simply isn’t true. Truly, ‘reality defying’.
As if the Past Five Years Never Happened
Investigative journalist Hannah Barnes, author of Time to Think, described listening to the WEC session as being like travelling back in time. It really was. Listening to Butler and Giordano wheel out long debunked myths about gender related distress, it felt as though the shameful safeguarding failures of the Tavistock, the damning testimony of a succession of GIDS whistleblowers and the landmark Cass Review had simply never happened.
I think it’s important that we get the facts on the record so, with the help of Professor Michael Biggs, I’ve fact checked the most egregious claims made by Professors Butler and Giordano. They may want to keep living in the past, but those of us who want holistic, evidence-based care for gender distressed young people are not going to let them take us backwards.
Claim #1: Professor Butler
“The GIDS was a specialist service set up to review the young people there and to explore what actually went on within their background, their history, their family, and their social environment. That was usually quite an extensive review. According to the service specifications, there were four to six sessions over a minimum of six months, but often many years, particularly for the presenting young people.”
Fact Check: It has been well established that the GIDS assessment service was wholly inadequate. This is extensively documented in Hannah Barne’s book Time to Think but is also evidenced in the 2020 CQC review of GIDS, which rated the service inadequate. In particular, the CQC report shows that assessments were sometimes completed in only two sessions, which directly contradicts Professor Butler’s testimony. The CQC described GIDS assessments as “unstructured, inconsistent and poorly recorded”, stating that “Staff did not develop holistic care plans for young people” and that the service did not “assess and manage risk well”. This included failing to record risk information about GIDS patients who were known to be self-harming or experiencing suicidal thoughts. It is not correct to state that GIDS patients were extensively or thoroughly assessed.
Claim #2: Professor Butler
“A small proportion of young people who had persistent gender dysphoria, which is a clinical diagnosis according to standardised processes of being a major discomfort with their gender being different from their biological gender, could then be referred to one of two endocrine clinics either in UCLH London or Leeds Children’s Hospital.”
Fact Check: Around 45% of young people seen by GIDS are believed to have been referred to endocrinology for puberty blockers.[1] This is not “a small proportion”. Professor Butler’s testimony seems to imply that only young people with childhood-onset of symptoms were considered for puberty blocking treatment. We know this is not true. Young people with recent onset of symptoms in adolescence, who came to make up the majority of the GIDS patient cohort, were regularly referred for blockers. Professor Butler appears to be trying to conflate early-onset of symptoms with the notion of ‘persistence’. In fact, using the DSM-5 diagnosis of gender dysphoria, GIDS considered young people to have “persistent gender dysphoria” if they had felt distressed about their sex for just six months.
Claim #3: Professor Butler
“We know very well from studies in the field on using the treatment for precocious puberty—which I have conducted in my previous history—that the hormonal process from the signals or hormones from the brain, the hypothalamus, to the pituitary gland and then to the testicles or ovaries starts again…We know that it is very unusual from follow-up studies with children who have received it for precocious puberty that there are no ill health effects in the long term nor are there any negative effects on fertility recovery.”
“Hence, from the paediatric endocrinology perspective, and I am not just speaking for myself, we do not see why outside the psychosocial side, in and around the gender side, there would necessarily be any other medical concerns to be considered around using puberty blockers in an adolescent who is otherwise healthy”.
Fact Check: Throughout his testimony, Professor Butler presented information about the safety of puberty blockers in treating precocious puberty as though this information also applied to their use in treating gender related distress in teenagers. These are completely different indications for use, as Dr Hilary Cass explained to the House of Lords in December 2024: “We are confident about that use [precocious puberty] because we have many years of experience, and because it is a very different situation from prescribing for young people with gender dysphoria. The difference is that children with precocious puberty have an abnormal hormone environment, which we normalise, whereas in young people with gender dysphoria we are taking a normal surge in pubertal hormones and disrupting it. That is why it is much less clear what the long-term impact of that intervention is”.
Claim #4: Professor Butler
“In the main, it is recognised as a reversible treatment. Certainly, again from my clinical studies and those we followed up who have had treatment for precocious puberty, I cannot recall a case where puberty did not restart.”
Fact Check: As outlined in Fact Check #3 above, the evidence on use of puberty blockers for precocious puberty does not apply to their use for gender related distress. To quote the Cass Review: “In the former case [precocious puberty], puberty blockers are blocking hormones that are abnormally high for, say, a 7-year-old, whereas in the latter they are blocking the normal rise in hormones that should be occurring into teenage years, and which is essential for psychosexual and other developmental processes” (Cass Review. 2024, p.174).
Professor Butler’s testimony here seems to imply that the only measure of reversibility is whether or not puberty resumes when blockers are stopped. The Cass Review identified this as a problem with the existing evidence base: it has tended to look only at whether treatment does or does not have the effect of physically suppressing puberty (Cass Review. 2024, p.175). But puberty blockers do not just physically stop puberty. They cause low bone density[2], prevent sexual development[3], disrupt cognitive maturation[4] and have been found to be associated with declining executive function in those who take them for more than one year[5] (Ibid. 2024, p.178). As the Cass Review makes clear, we have no long term data that could tell us whether or not these effects are reversible.
Claim #5: Professor Butler
“If you are taking steps to slow down puberty, the bone mineral content, which is the amount of calcium in the bones, is carefully monitored and it is routine part and parcel of the assessments there.”
Fact Check: Analysing Professor Butler’s own data, Professor Michael Biggs has shown that 1 in 6 young people undergoing puberty suppression have concerningly low bone density, compared to 1 in 770 in the general population. Despite this deeply concerning figure, the NHS checks the bone mineral content of young people taking puberty blockers only once per year. This can hardly be described as ‘careful monitoring’. Amazingly however, Professor Butler has argued that even annual monitoring is unnecessary, writing in 2019 that: “that yearly DXA scans [the x-ray scans used to measure bone density] may be unnecessary .... Yearly DXA scans can be a large expense to service providers.”
Claim #6: Professor Butler
“When you instigate puberty blockers in a trans young person, there is a delay of the calcium going into the bones. It does not actually reduce, it just stands still and does not increase quite as quickly. However, what we know from follow-up studies which have been published from Amsterdam— and what we in the UK are about to publish soon—is that that bone calcium content recovers once sex hormones are started.”
Fact Check: The Amsterdam follow up study apparently cited here by Professor Butler does not in fact show that bone health recovers following cross sex hormone treatment. The Amsterdam gender clinic found that trans identified males continued to have low bone density in their spines even after over ten years of taking estrogen. Nine out of 25 of the transwomen in the Amsterdam sample had a spine Z-score below -2, meaning that they were at significant risk of developing osteoporosis.
Professor Butler was later asked by MP Rosie Duffield how he knew it to be true “that bone calcium content recovers once sex hormones are started”. He was obliged to clarify that: “My original comment was with children having precocious puberty treatments, not necessarily in the gender field.” So, once again, Professor Butler was presenting the evidence in relation to precocious puberty as though it were applicable to gender related distress. As outlined above, this is simply not the case. The Cass Review (2024, p.178) identified a need for “much longer-term follow-up…to determine whether there is full bone health recovery in adulthood”, so it is alarming to see Professor Butler misrepresenting the evidence on precocious puberty to claim that this is not an area of concern.
Claim #7: Professor Butler
“Things that are important and which we always assess are appropriate nutrition, vitamin D, and exercise.”
“It is probably different from adult practice, but in children and young people the first thing is to ensure they are eating well and appropriately with adequate nutritional balance, particularly calcium in the diet. We always ensure that young people on those treatments will have vitamin D supplementation, which is not an exceptional thing for recommendation for adolescent health, and that they partake in physical exercise where possible because that is also noted to promote bone health.”
Fact Check: These comments, which suggest that very low bone density can be managed through diet and exercise, are difficult to square with the very serious levels of degradation to bone health identified by Professor Michael Biggs. Some young people treated with puberty blockers have bone density so low that they are at highly elevated risk of developing osteoporosis. It seems unlikely that the risks associated with such severely low bone density can be successfully mitigated through diet and exercise.
Claim #8: Professor Giordano
“The other concern is around the brain development. Animal studies suggest that sex hormones affect brain changes. One question is whether this would be true for humans as well. Of course, we cannot do the same studies on humans that we would be able to do on animals. Studies have looked at what can be looked at: cognitive functioning, executive functioning and IQ scores. Again, the scientists who have looked into this matter have found no difference in executive functioning, cognitive functioning and IQ scores of trans young people treated with puberty blockers compared to the cisgender cohorts.”
Fact Check: The unwarranted certainty with which Professor Giordano made these assertions is deeply concerning. The Cass Review (2024, p.178) found “very limited research “on the short-, medium- or longer-term impact of puberty blockers on neurocognitive development” and stated that “brain maturation may be temporarily or permanently disrupted by the use of puberty blockers, which could have a significant impact on the young person’s ability to make complex risk-laden decisions, as well as having possible longer term neuropsychological consequences.”
A 2024 systematic review found evidence that puberty blockers may have “a detrimental impact…on IQ”, while the Cass Review (2024, p.178) identified a cross-sectional study that found “worse executive functioning in those treated [with puberty blockers] for more than one year compared to those not treated”.
It is deeply alarming that Professor Giordano failed to make the committee aware of these well documented findings and the grave uncertainty that surrounds the impact of puberty blockers on brain development.
Claim #9: Professor Giordano
“We need to be very careful about the side effects, the known and potential side effects, of the treatment that we provide, and that is missing out the consideration of what happens to the young person if they do not receive the medication which, incidentally, is also a big part of the legal reasoning about the treatment of children…So, judges said clinicians need to consider what would happen to young people if they did not receive medical treatment…Can this person live satisfactorily without medical intervention, or is the dysphoria so significant that it will cause mood disorders similar to mood disorders that would be caused to young people who suffer from precocious puberty, anxiety and depression? Would they be able to attend school? Would they be able to integrate with other people? Would they become suicidal?
Fact Check: Thankfully, suicidality is one area of paediatric gender medicine in which we have very solid evidence. The comprehensive and careful work of Professor Louis Appleby, the government’s own expert advisor on suicide, has demonstrated that gender distressed young people are at no greater risk of suicide than their peers with equivalent mental health conditions. This has also been confirmed by the Cass Review (2024, p.186-187), which found that “suicide risk appears to be comparable to other young people with a similar range of mental health and psychosocial challenges” and further highlighted that “the evidence does not adequately support the claim that gender affirming treatment reduces suicide risk.”
Professor Giordano’s comments actively invite young people to consider themselves at risk of dire harm if they are unable to access puberty blockers. In particular, they directly contravene the Samaritans guidelines on safe reporting of suicide by suggesting that suicidality may be caused by a single event or factor (inability to obtain puberty blockers) and by addressing young people, the demographic group most susceptible to suicide contagion. This is completely unacceptable, especially given the particular care taken by Health Secretary Wes Streeting to speak directly to young people and reassure them that the ban is a safety measure that does not mean they will be left to manage their distress alone.
There is no evidence to support Professor Giordano’s assertions that going through natural puberty worsens gender dysphoria, causes mood disorders or prevents young people from attending school or integrating with their peers. Many of the current cohort of young people presenting to gender clinics have anxiety, depression and problems with psychosocial functioning that predate any experience of gender related distress. It has been theorised that gender related distress may actually be part of the symptom profile of these underlying conditions, rather than a discrete syndrome in and of itself. It is well established both that feelings of gender related distress resolve after natural puberty for the majority of young people who are not medicalised (Cass Review. 2024, p.64) , and that puberty blockers do not reduce gender dysphoria (Ibid. 2024, p.176) or relieve co-occurring mental health conditions (Ibid. 2024, p.176-177). In fact, reanalysis of the GIDS Early Intervention Study (EIS) shows that 71% of young people whose puberty is blocked actually experience declining mental health (34%) or no change in their mental state (37%).
Professor Giordano’s perpetuation of the suicide myth, which has provoked so much fear among young people and their families, should on its own surely disqualify her from any further professional engagement on this subject.
Claim #10: Professor Giordano and Professor Butler
Professor Giordano: “In the literature, there is no reported case of complaint around loss of mineral density from the cohort of children treated since the mid-1990s. There is no report in the literature, no litigation, no complaint through clinical authorities from patients.”
Professor Butler: “Breaking is very unusual to happen in adolescence…that is not something that we would see because the bone, even if there is a change in bone density, rarely gets below the range or into the range you would expect fractures to occur.”
Fact Check: This is untrue. The Karolinska Clinic in Stockholm reported in 2022 that it had received three patient complaints involving bone density. This included a child treated with puberty blockers for four years who had developed osteoporosis, reporting constant pain in their back and hips. In Hannah Barne’s book Time to Think, one young GIDS patient treated with puberty blockers reported having broken four bones while undergoing treatment[6].
Claim #11: Professor Butler
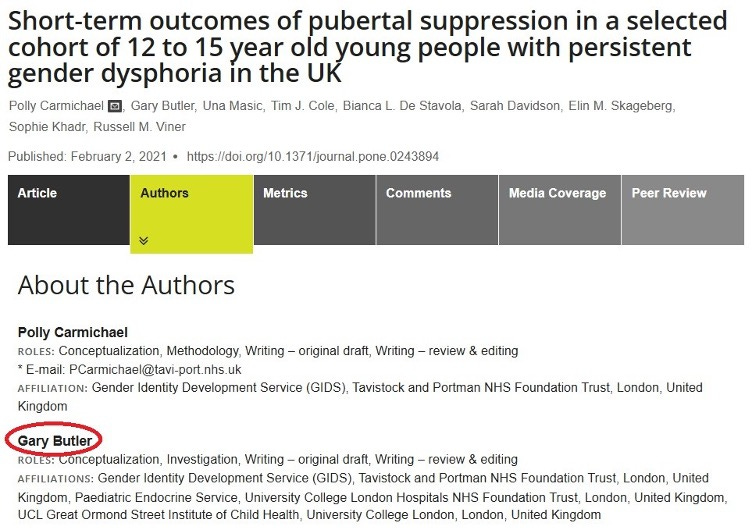
Rosie Duffield: “Can I just ask you about your time at the GIDS? Why did you continue to prescribe puberty blockers when the preliminary results from the early intervention study in 2015, 2016 which, of course, you were heavily involved with, did not demonstrate clear benefit?”
Professor Butler: “At that stage, the contract was within NHS England, which provided the framework for the service specifications. The contract was then with the GIDS at the Tavistock, and the endocrine clinics provided support from that. So, that was within the bodies and within the NHS England service specifications and its commissioning.”
Rosie Duffield: “Why were the results not published until 2020?”
Professor Butler: “I was not directly involved in that study myself”.
Fact Check: As the image below shows, Professor Butler is listed as one of the authors of the GIDS EIS. His roles are described as “Conceptualization, Investigation, Writing – original draft, Writing – review and editing”. Given that he was therefore involved in quite literally every part of the EIS, it is extremely difficult to understand his claim that he “was not directly involved”.
Claim #12: Professor Giordano
“First, on the conveyor belt concern. I cannot comment on how the services were stretched and how the assessment was carried out because I was not part of that. However, the international consensus and the recognised practice is to consider puberty blockers as a complement of a number of other psychosocial measures only in those cases where the young person suffers from what was called until recently strong and persistent gender dysphoria that would not be alleviated by other means.”
Fact Check: We can only assume that Professor Giordano is referring to the disgraced WPATH Standards of Care 8 (SOC8) when she refers to ‘international consensus’ and ‘recognised practice’. WPATH does not advise that young people take puberty blockers only “as a complement of a number of other psychosocial measures” or recommend that young people engage in extensive psychological therapy before commencing treatment. In fact, WPATH advises clinicians only to address young people’s co-occurring mental health needs if they are seen to “interfere with diagnostic clarity” or “capacity to consent”.
While Professor Giordano states that she cannot speak to practice at GIDS, the service repeatedly stated that it did not provide therapy and was there only to provide an assessment leading to a referral to endocrinology[7]. After commencing puberty blockers, GIDS actually saw patients less often, meaning that they were certainly not receiving other forms of psychosocial support[8]. Whistleblowers have repeatedly highlighted that GIDS was in fact a ‘conveyor belt’ towards medicalisation.
As mentioned earlier, the DSM-5 only requires that young people experience symptoms of gender related distress for six months before they qualify for an official diagnosis of gender dysphoria. It is misleading to suggest that young people have typically been carefully screened for “strong and persistent gender dysphoria” prior to being referred for puberty blockers, or that they have been provided as a ‘complement’ to other treatments.
Claim #13: Professor Giordano
“My second point concerns the benefit and your claim, Ms Duffield, that the study of that cohort published from the clinical trial concerning Tavistock did not show benefits. To say that puberty blockers do not have benefits in terms of suspending puberty is like denying that the earth is spherical. For someone who is distressed by pubertal development, suspending pubertal development is clearly a benefit.”
Fact Check: Professor Giordano here attempts to restrict our understanding of ‘benefits’ to whether or not puberty is effectively suppressed. This can only be regarded as a ‘benefit’ if we agree with Professor Giordano that blocking puberty is an appropriate way to respond to a young person’s feelings of distress about adolescence.
An alternative view regards puberty blockers as preventing the very developmental processes that typically lead to resolution of gender related distress. In particular, puberty blockers halt sexual development, thereby preventing young people from developing an understanding of their own sexual orientation and resolving any discomfort or conflict they may feel about this. It is important to remember that almost 90% of gender dysphoric young people can expect to experience resolution of their symptoms after puberty if they do not take blockers. By contrast, we know that 98% will go on to take sterilising cross sex hormones if they do take puberty blockers.
Avoidance is not a psychologically healthy way to teach young people to manage feelings of distress, particularly when it involves taking experimental medications with unknown long term effects. It can be helpful to consider whether we would encourage young people to adopt a similar avoidance strategy in the face of other distressing feelings. There can be no doubt that young people with anorexia are deeply distressed by their weight. Should we facilitate them to take weight loss drugs or get liposuction? If, as Professor Giordano suggests, we severely limit our understanding of ‘benefit’ by looking only at how the young person feels about their weight, then we might give them a prescription for Ozempic or a referral for surgery. But, if we take a holistic view of the young person’s wellbeing, we would surely conclude that they need compassionate support to understand and manage the underlying causes of their distress. Replace ‘anorexia’ with ‘gender related distress’ and ‘liposuction’ with ‘puberty blockers’ and it becomes clear that the question of ‘benefits’ is far more complex than Professor Giordano makes out.
Claim #14: Professor Giordano
The question is whether that benefit outweighs the risks and whether that benefit is justified. When the measures of benefits are taken, sometimes they are taken in a questionable way. For example, the York study compared people before and after taking puberty blockers and found that their mental health did not improve or get worse. They concluded that therefore there was no need to give puberty blockers, and that conclusion fed into the Cass Review. But from a clinical perspective, you can predict that a dysphoric adolescent will get worse and worse mentally, so stability can be a good clinical outcome.
Fact Check: We cannot “predict that a dysphoric adolescent will get worse and worse mentally”. As outlined in Fact Check #13 above, up to 98% of young people with gender related distress experience resolution of symptoms after puberty if they do not receive blockers.
Professor Giordano appears to be referencing the GIDS EIS, which found that 34% of young people treated with puberty blockers experienced declining mental health, while a further 37% experienced no change. This means that almost three quarters of children either got worse or received no benefits from undergoing risky, experimental treatment. It is quite a stretch for Professor Giordano to frame ‘no change’ as evidence of ‘stability’ considering the risks and unknowns associated with puberty blockers, particularly given the widespread availability of alternative treatment modalities that could safely be used to manage feelings of distress.
Claim #15: Professor Giordano
“The same applies when people assume puberty blockers are not beneficial because they do not have any statistically significant impact on gender dysphoria. That is not what puberty blockers are intended for. They are not a treatment for gender dysphoria. If you measure the effect or benefits of puberty blockers on the reduction of gender dysphoria, you are clearly not going to find a benefit there.”
Fact Check: This raises the question of what Professor Giordano believes the rationale for treatment with puberty blockers actually is, given their experimental use in the treatment of gender related distress and their multiple adverse side effects. As we saw above, she concedes that they do not improve mental health, albeit with the strange caveat that she regards ‘no change’ as a beneficial outcome.
If puberty blockers do not improve mental health or gender dysphoria, then the only justification for their use would appear to be that they reduce puberty anxiety while a young person decides whether or not to take sterilising cross sex hormones. Professor Giordano appears to be recycling the disproven thesis that puberty blockers buy “time to think”, about which the Cass Review (2024, p.176) said:
“puberty blockers are not buying time to think, given that the vast majority of those who start puberty suppression continue to masculinising/feminising hormones, particularly if they start earlier in puberty.”
Claim #16: Professor Butler
“Within endocrinology, very little has a licence for use in children, including growth hormones and puberty blockers. There are general guidelines, usually national, specialist or scientific society guidelines and international guidelines as well, and it is expected that we would refer to those in the use of treatments such as sex hormone treatments”.
Fact Check: The Cass Review (2024, p.130) identified “serious questions about the reliability of current guidelines”, identifying only two national guidelines from Finland and Sweden that “could be recommended for use in practice”.
Claim #17: Professor Giordano
“Use for a different indication might be experimental at the very start, although in this particular case, the cohort was remarkably similar to the central precocious puberty cohort in that it still concerned adolescents and was intended for the purpose of delaying pubertal development”.
Fact Check: The cohorts are not “remarkably similar”, as detailed in the statements made by Dr Hillary Cass listed in Fact Checks #3 and #4 above.
Claim #18: Professor Butler
“When a treatment is prescribed or recommended off-label, the onus is on the prescriber to ensure monitoring of efficacy and outcomes. That is exactly what we do in our routine practice for any medication given to children and young people, but in this field especially we have very extensive information around monitoring the welfare of these young people.”
“We have a more extensive evaluation and monitoring process specifically with puberty blockers than we would for a child with precocious puberty… We would often do more blood tests, more physical checks, more assessment of bone health and obviously in parallel with our psychometric colleagues, we would assess their mental health as well.”
Fact Check: This is complete nonsense. We know that children taking puberty blockers were not carefully monitored by GIDS. In fact, GIDS saw them less frequently after they commenced endocrine treatment[9].
If Professor Butler can produce “very extensive information around…the welfare of young people” who have been treated with puberty blockers over the last twenty years then there is an urgent need for him to make it public. GIDS were unable to produce such data when it was requested by the High Court in Bell v Tavistock and the Cass Review identified no such information. We really have no idea at all what has happened to the young people prescribed puberty blockers by Professor Butler and his colleagues.
Claim #19: Professor Giordano
“So, there are a number of peculiarities that follow from the provision of medical treatment only within a research trial, which could be circumvented by providing treatment to all patients for whom the benefits ratio is similarly favourable and then engaging in research on a voluntary basis with long-term follow-ups.”
Fact Check: This is essentially to say that the puberty blocker ban should be rescinded, the treatment should continue to be available to everyone despite its known risks and experimental status and that no systematic efforts to collect evidence on its effects should be undertaken. Professor Giordano is essentially arguing that we should reset the clock to 2005 and continue treating young people according to a model of care found to be unsafe by the Cass Review, the CQC and the Commission for Human Medicines.
Claim #20: Professor Butler
“I do not know whether you and members of the Committee are familiar with people who are transgender or living their lives differently from their birth gender, but as someone who has had clinical experience in this area, the distress and anxiety in the young person and their families is very, very clear in the majority. Many of them at that time are just not functioning despite psychological help or support. If one can provide that form of respite to prevent or reduce the physical changes and functions that are causing the dysphoria, then that can restore the function of the young person and the family in that regard.”
Fact Check: It is not correct to state that puberty blockers “restore the function of the young person”. As outlined above, the GIDS EIS found that mental health either worsened or did not change for 71% of children treated with puberty blockers. The Cass Review (2024, p.176) states that:
The University of York concluded that there is insufficient and/or inconsistent evidence about the effects of puberty suppression on psychological or psychosocial health. This is in line with the finding of the NICE review (2020) and other systematic reviews.
Claim #21: Professor Butler
“We wrote a review commentary on this some years back about how when your back is against the wall it is very difficult not to be able to provide help where help is available.”
Fact Check: It is not acceptable to provide a risky, experimental treatment to distressed young people on the basis that it is emotionally difficult for clinicians to witness their distress or correct their misapprehensions about the safety and efficacy of the treatment. The fact that young people have been misled into thinking that puberty blockers are ‘lifesaving’ does not give clinicians a license to collude in perpetuating this misapprehension now that we know it is not true. Professionals who feel that their “back is against the wall” when faced with a gender distressed young person are ignoring multiple, evidence-based treatment modalities known to help alleviate and manage distress.
Claim #22: Professor Giordano
“a clinical trial that is the only way to obtain a medication that is felt as necessary by many trans people and their families, is already, by default, vitiating the informed consent process.”
Fact Check: Declining to provide an experimental medical treatment outside the terms of a clinical trial, when that treatment is known to be neither safe nor effective, is not a violation of the informed consent process. According to this view, all that is necessary for informed consent is that the patient feels the medication is necessary. Professor Giordano appears to believe that it is irrelevant whether the medication is objectively necessary, safe or effective.
If a person feels that chemotherapy is the necessary treatment for their eczema, is the doctor “vitiating the informed consent process” by refusing to provide it? Of course not. If a patient is labouring under a misapprehension about the safety or efficacy of a treatment then the role of the clinician is to sensitively correct those misapprehensions and explore alternative treatments.
Claim #23: Professor Giordano
“In this case, it is quite interesting because it is not the medication per se that is banned but the application. Endocrinologists can continue to prescribe that medication off-licence for adolescents with endometriosis, or precocious puberty on-licence, but not for gender dysphoria. That is quite a peculiar situation.”
Fact Check: There is nothing even slightly remarkable about this. If a culture had arisen in which doctors were treating eczema using chemotherapy, and it had been realised that there was no evidence for this and that it was producing serious adverse outcomes, it would be perfectly reasonable to ban chemotherapy for the application of treating eczema while leaving it available for the treatment of cancer.
Claim #24: Professor Giordano
“In this case, there is no evidence of lack of safety. There are legitimate concerns, but concerns are not evidence… It is quite peculiar to me that it is not the drug but the application that has been banned not on grounds of safety, but on grounds of concerns, however legitimate”
Fact Check: I don’t know how Keira Bell felt, as she heard Professor Giordano describe the experience of detransition and regret as merely a ‘concern’, but I think I would have found it really upsetting. Keira, and other young people treated with these drugs, have testified to the devastating regret they feel and the irreversible harms they have experienced as a result.
It is quite remarkable to claim that “there is no evidence of lack of safety”, given the testimonies of those young people, the extensive evidence of harm found by the Cass Review and the verdict of the Commission on Human Medicines that there is an “unsafe prescribing environment” for these drugs.
Claim #25: Professor Giordano
“We also need to accept that in this area of medicine, as in many other areas of medicine, we might not achieve that GRADE 1 evidence. It is perhaps necessary to change the goalposts and to accept that some areas of medicine have such vast repercussions in people’s lives that what we want to measure is so nuanced it cannot fit into that scale of GRADE. It is also ethically problematic to withhold medical treatment that is experienced as beneficial and that nobody has complained about on grounds that there is not enough evidence yet, if what is meant by evidence is unattainable.”
Fact Check: On one of the points Professor Giordano made here, we actually agree! It simply isn’t possible to generate GRADE 1 evidence about the use of these drugs. There is no way to adequately blind a trial and studies that don’t have a control group will only produce more inadequate and uncertain evidence. We also think a puberty blocker trial will be powerfully culturally contingent: the current narrative about transgender identity, and particularly the mistaken belief that puberty blockers are ‘lifesaving’, is likely to significantly bias the results in ways we can’t control for. As Dr Louise Irvine, co-chair of the Clinical Advisory Network on Sex and Gender recently said in a Genspect UK webinar, it simply isn’t ethical to carry out risky research on children when we know that research won’t generate meaningful results. This is especially so when we know that most young people experience resolution of symptoms without medical intervention and when there are multiple, safer treatments for managing distress available.
Two Fundamental Disagreements
However, we powerfully disagree with Professor Giordano on two points. The first is about what should be done when patients demand access to a dangerous medication which has unknown long term effects and is associated with mounting evidence of harm. Professor Giordano argues that we should simply abandon efforts to do research and prescribe puberty blockers to any young person who feels they need them. As outlined in Fact Check #22 above, we don’t believe that a patient’s subjective feelings about a treatment should dictate its availability when there is objective evidence of adverse effects. It’s also not true, as outlined in Fact Check #24, that “nobody has complained” about puberty blockers. Keira Bell was seated right behind Professor Giordano when she made this astonishing claim.
Instead, we believe responsible clinicians have a duty to educate their patients and the public about the risks and harms associated with puberty blockers. We need to roll back the misinformation that has been spread by activists and relieve some of the fear felt by the gender distressed young people they have lied to. Clinicians can offer young people hope by providing evidence based treatments to manage their distress, rather than amplifying their fears by reciting misinformation, as Professors Butler and Giordano did throughout the WEC session. There is actually a need for extensive research, just not on the effects of medicalising gender related distress. We need to trial non-medical approaches, investigate the aeitology of the condition in the new cohort and begin to understand its co-occurrence with autism, in addition to unpicking the influence of factors like social media and pornography.
Our second disagreement with Professor Giordano concerns the notion that a treatment can have “vast repercussions in people’s lives” while simultaneously being so ‘nuanced’ that it defies objective measurement. If an intervention has ‘vast repercussions’ we would expect these to be clearly reflected in substantially improved outcome measures across the short, medium and long term, even if the evidence did not reach GRADE 1 standard. Instead, the University of York systematic review found that “No conclusions can be drawn about the effect [of puberty blockers] on gender-related outcomes, psychological and psychosocial health, cognitive development or fertility”.
If puberty blockers have “vast repercussions in people’s lives” we would expect thirty years of research on their use to have produced at least some systematic evidence of improvements according to these measures. In fact, as the Cass Review (2024, p.176-177) makes clear, none of the proposed benefits of puberty blockers (buying “time to think”, reducing gender dysphoria, improving psychological and psychosocial wellbeing and cosmetic outcomes) are currently supported by evidence. This is not because the benefits of puberty blockers are ‘nuanced’. It is because this is a failed medical intervention which does not substantially improve the lives of people who take it.
Nothing More than Feelings
Suggesting that we simply cannot say what constitutes a benefit or a risk in relation to this treatment and these patients is highly relativistic, and exceptionalises gender distressed young people by implying that ordinary measures of risk, benefit and safety do not apply to them. The Cass Review was critical of this approach, but Professor Giordano’s publication history suggests that problematising conventional notions of ‘good’ and ‘bad’, in order to argue that the subjective perceptions of the individual should override objective clinical decision making, has been a central focus of her academic career. She has written extensively about the question of whether patients with severe anorexia should be allowed to decline lifesaving medical treatment when it is foreseeable that this will lead to their death, thereby effectively assisting them to commit suicide. Giordano’s view is that:
Whether or not anorexics should be allowed to die depends not primarily on their competence…but on the extent of their suffering and on whether it can be alleviated.
We can see that it is not unusual for Professor Giordano to argue that the subjective feelings of the patient (including about the likely efficacy of treatment) should be given priority over careful clinical decision making, even when that may lead to the preventable death of the patient. In academic circles, a certain amount of prestige may attach to being on the radical side of abstract debates about individual autonomy and harm. But in the real world, very vulnerable people, especially young people, often need to be protected from making decisions that are not in their best interests. It is notable that Professor Giordano is not a medical professional, and therefore has limited experience of dealing with the lived reality of treating complex conditions, like anorexia and gender related distress, where multiple intersecting factors may severely limit a patient’s competency to consent.
[1] Barnes, H. 2020, p.282. Time to Think.
[2] “Multiple studies included in the systematic review of puberty suppression…found that bone density is compromised during puberty suppression…much longer-term follow-up is needed to determine whether there is full bone health recovery in adulthood”.
[3] “Blocking this experience means that young people have to understand their identity and sexuality based only on their discomfort about puberty…Therefore, there is no way of knowing whether the normal trajectory of the sexual and gender identity may be permanently altered.”
[4] “brain maturation may be temporarily or permanently disrupted by the use of puberty blockers, which could have a significant impact on the young person’s ability to make complex risk-laden decisions, as well as having possible longer term neuropsychological consequences.”
[5] “worse executive functioning in those treated [with puberty blockers] for more than one year compared to those not treated”.
[6] Barnes, H. 2020, p.214-215. Time to Think.
[7] Barnes, H. 2020, p. 154-155. Time to Think.
[8] Ibid. 2020, p.73.
[9] Barnes, H. 2020, p.73. Time to Think.
Does anyone know who are the muppets on the WEC?